- What is CIRS?
- How Serious Is This?
- What Does CIRS Do To The Body?
- Why Don’t People Know About This Already?
- How to get diagnosed:
- Symptom Clusters (more than 8 of these is positive for CIRS):
- Common Misdiagnoses and Other symptoms you might recognize:
- CIRS Tests:
- CIRS blood work usually includes:
- Other CIRS tests and common results:
- VCS (Visual Contrast Sensitivity) Testing:
- How VCS Testing Works:
- MARCoNS (Multiple Antibiotic Resistant Coagulase Negative Staphylococci):
- NeuroQuant:
- Blood Markers:
- Genes/Genetic susceptibility:
- CIRS HLA Susceptible Haplotypes:
- alpha-MSH (Melanocyte Stimulating Hormone):
- TGF beta-1:
- Complement C4a:
- MMP-9 (Matrix Metalloproteinase-9):
- ADH/Osmolality (Vasopressin):
- ACTH (Adrenocorticotropic Hormone)/Cortisol:
- Leptin:
- VEGF (Vascular Endothelial Growth Factor):
- Anti-Gliadin Antibodies:
- VIP (vasoactive intestinal peptide):
- vWF (von Willebrand Syndrome):
- Vitamin D:
- Plasminogen activator inhibitor-1 (PAI-1):
- Pulmonary Hypertension:
- VO2 Max:
- POTS and PANS:
- GENIE:
- Treatment
- 1. Removal From Exposure:
- ERMI/HERTSMI-2 testing for molds:
- Ineffective Testing:
- Companies:
- 2. Binders:
- Cholestyramine (CSM) (or Welchol) (prescription):
- Other Binders:
- Also 2. Fish Oil:
- Also 2. Diet:
- 3. MARCoNS
- 4. Possibly some of these are necessary:
- DDAVP:
- Actos:
- Losartan:
- DHEA:
- 5. VIP (Vasoactive intestinal polypeptide):
- Definitions:
- Gene Definitions:
- Alleles:
- Chromosome:
- Gene:
- Haplotypes:
- HLA:
- Immune System Definitions:
- HLA-DR/DQ:
- MHC class I:
- MHC class II cell surface receptor:
- Peptide:
- Antigen:
- Antibody:
- B cells:
- T cells:
- Adaptive immune system:
- Complement system:
- Lymphocyte:
- Cytokines:
- Chemokines:
- Biotoxins:
- Current CIRS biotoxins:
- Blood brain barrier (BBB):
- Capillary hypoperfusion:
- PASP (pulmonary artery systolic pressure):
- TR (tricuspid regurgitation):
- TRPV:
- Genetics:
- Genomics/Transcriptomics:
- Proteomics:
- Metabalome:
- Nanostring:
- GENIE (Genomic Expression by Nanostring: Inflammation Explained):
- References
This is the overview I wrote for biotoxins and CIRS. It's extensive but it covers everything I've learned as well as the questions I had (although there's more info under Treatment and FAQ and Scientific Articles). This is for someone who wants to read and fully understand the severity of biotoxins. If you're not interested in the science behind it, go straight to Treatment. You can use the Table of Contents on the right to stay organized on here.
What is CIRS?
CIRS stands for Chronic Inflammatory Response Syndrome, named by Dr. Shoemaker. It occurs to genetically predisposed people (24% of the population) after somewhat chronic exposure to water damaged buildings, or exposure to other biotoxins (certain types of algae, Pfiesteria, Lyme bacteria, more on that below). You wouldn’t necessarily put yourself in this category except a whopping 80% of houses have water damaged. So you probably have had chronic exposure, and if you’re genetically predisposed you probably have issues from that exposure.
Symptoms are wide ranging but involve multiple organs. Genetically predisposed people make up 95% of the patients that have CIRS. 24% of the population has genes that predispose them to CIRS. Like I said, the terrifying part of this is 80% of buildings are water damaged. 50% have current water damage and 30% have previous water damage that has caused mold/bacteria growth at some point. Water damage can come from any type of flood including a pipe leak or bathroom leak, an overflowing tub or sink, appliances, or roofing issues. Basements and attics are very prone to mold growth. Mold growth is a simplification. CIRS is mostly caused by bacterial growth in water damage (can be associated with a musty smell), mycotoxins from mold are actually only a small part of the issue. A lot of the growth of these organisms are in HVACs or behind walls. Mold/bacteria only need 24-48 hours of damp conditions to grow, and in highly humid areas, growth in HVACs is basically inevitable. Very ill people may also get sick from full neighborhoods due to the bacteria and mold count in the air, particularly humid areas on the water, or valleys. Mold and bacteria growth occurs at a humidity level above 60% (so keeping your house at 50% humidity or lower is strongly advised).
How Serious Is This?
This is bad. This is very, very bad. In my opinion this is a bigger issue than other inhaled syndromes and diseases (smoking, asbestos, lead, etc.) that humanity has been exposed to in the last 150 years. This is not the first discovery of something in our living environments causing illnesses and death. Ergot - a fungi that grew on rye fields, caused nausea, vomiting, muscle pain and weakness, numbness, itching, and rapid or slow heartbeat. It could progress to gangrene, vision problems, confusion, spasms, convulsions, unconsciousness, and death and decimated entire towns in the Middle Ages and 1700’s (LSD was invented using ergot). Asbestos was used in building materials and even clothes as a fire retardent. It still kills about 250k people per year. In the early 1900’s they realized that people who mined asbestos got sick but it wasn’t until the 1970’s that it was widely recognized that materials with asbestos led to disease and death. I had old great aunts and uncles die from asbestos poisoning. Then there’s lead. Lead toxicity has been known since 200 BC… but it was still added to paint to speed up drying, and it was used in gasoline to stop engine knocking. It wasn’t until the 1970’s that the government phased out lead in gasoline and it wasn’t until 1978 that the government banned lead in paint. It’s still in the paint of a lot of buildings built before 1978.
Although CIRS has been around forever, a few things happened to buildings that made biotoxins deadlier than before. In the 1940’s drywall was introduced. After the 1950’s this was basically how homes were made instead of using plaster. Drywall is basically paper. If paper gets wet, it gets moldy. Drywall is way worse for damp conditions than plaster, it’s porous. Mold/bacteria can grow on the back, in it, in areas you can’t see. It is really not suitable for building houses. Then in the late 1980’s and early 1990’s, antifungals were added to paint to inhibit mold growth because drywall is so prone to mold. Those antifungals have created super fungi (like antibiotics have created antibiotic resistant bacteria).1 Instead of having molds that can be okay, or somewhat problematic, we have molds that are extremely toxic, thriving on walls that they can survive on. Antifungals were also added for food productions, agricultural purposes (crops, etc.), pharmaceutical preparations, starting in the 1950’s with more and more use which has bred more toxic fungi (like antibiotics have bred antibiotic resistant more toxic bacteria).2
In humid areas this is even more of a nightmare. And most places are humid. In order to solve this problem, building materials need to be updated and drywall needs to stop being used or this isn’t going to get better.
Since CIRS is coming to light, there have been a number of successful legal cases involving very sick CIRS patients, and some news articles about it from all around the world. There would be a lot more if it weren’t misdiagnosed 99% of the time.
https://www.express.co.uk/life-style/health/1709442/mould-toxicity-symptoms-tingling-numbness-hands
What Does CIRS Do To The Body?
To put it bluntly, it screws up your entire body and then you end up dying eventually of something like Parkinson’s or Alzheimers. Like I said, this is really bad.
CIRS occurs when the innate immune system doesn’t interact with the adaptive immune system properly due to poor antigen presentation and there’s a generally chronic exposure to biotoxins, usually in water damaged buildings (although other exposure does trigger CIRS). This means that the adaptive immune system isn’t activated properly leading to a fairly permanent activation of the innate immune system and consequent multi-organ tissue damage from inflammation and pathogens that aren’t excreted. Biotoxins that cause CIRS cause their own damage in the body as well, and turn genes on that wreak havoc separate from the inflammatory response. See FAQ for more in-depth information. There are symptoms outlined below but CIRS can cause symptoms ranging from autoimmunity, allergies, migraines, chronic fatigue syndrome, psychiatric illnesses, to autism in children, to Parkinsons and Alzheimers and Dementia and ALS. This is what makes it so scary. Under papers at the bottom are links to peer reviewed articles showing these diseases caused by inhaling biotoxins, and resolution of these diseases with CIRS treatment. It’s absolutely insane. This overview isn’t meant to fearmonger, if anything it’s meant to bring hope to people suffering but my warning is:
Do Not Ignore This.
There is a 24% likelihood that you have a genetic predisposition that (if chronically exposed to one of the 80% of buildings with water damage) can lead to an extremely nasty death long term, and a lot of suffering before that. And this is not the type of suffering that diet alone will cure. Fortunately there’s a treatment, and even if you’ve been sick for your whole life, there’s peer reviewed evidence that you can still heal with CIRS treatment.
Why Don’t People Know About This Already?
Unfortunately for me (and for 24% of the world), this is a fairly new discovery. It’s like discovering asbestos and lead causing disease. It’s just new. The oldest studies are from 1997 and it wasn’t even formally named until 2003 (peer reviewed studies for the treatment protocol from then). The only reason people don’t know about this is because it’s new. It’s certainly not for lack of research though.
CIRS also isn’t easily recognized by the medical system because they don’t normally test the innate immune system markers, they test the adaptive immune system. CIRS symptoms are kind of all over the place as well, so misdiagnosis is extremely common. CIRS is usually caused by chronic exposure to WDB’s (water damaged buildings) but it can also be triggered by certain exposure to Lyme bacteria (causing chronic lyme after treatment), consumption of reef fish containing neurotoxins, algae blooms, and other biotoxins.
How to get diagnosed:
Go to FAQ for helpful links to find practitioners.
You need to have 8 or more symptoms, exposure to water damaged buildings or other toxins, genetic predisposition, and 4 of the blood markers seen in CIRS need to be wonky to be diagnosed. The carnivore diet does reduce the inflammatory response (paper being published soon).
Symptom Clusters (more than 8 of these is positive for CIRS):
- Fatigue
- Weakness, assimilation, aching, headache, light sensitivity
- Memory, word finding difficulties
- Concentration difficulty
- Joint pain, AM stiffness, muscle cramps
- Unusual skin sensations, tingling
- Shortness of breath, sinus congestion
- Cough, thirst, confusion
- Appetite swings, body temperature regulation problems (hot or cold), urinary urgency
- Red eyes, blurred vision, sweats, mood swings, ice pick pain
- Abdominal pain, diarrhea, numbness
- Tearing, disorientation, metallic taste
- Static shocks, vertigo (Static shocks occur due to rising salt levels in the blood due to dehydration. Salt is released onto the skin through the sweat glands and creates a battery-like effect that increases the electrostatic shock potential. Chloride levels may be higher than cystic fibrosis patients in some cases.)
Common Misdiagnoses and Other symptoms you might recognize:
- POTS (blacking out when standing up)
- PANS (kids)
- Urinary urgency (bed wetting or clothes wetting in kids)
- Dehydration (excessive thirst - adults and children)
- Depression (severe)
- Anxiety
- Asthma
- ADHD
- Fibromyalgia
- Mental disorders
- Autism
- Neurological diseases
- Hypothyroidism
- Parkinson's
- ALS
- Alzheimer’s
- Dementia
- Autoimmunity (MS, Lupus, Arthritis)
- Allergies to everything
- Digestive problems
- Long COVID
- GERD or acid reflux
- Fine resting tremor
- Volatility/rage randomly (e.g. punching walls)
- Muscle weakness (85% of CIRS patients)
A combination of VCS testing and symptom cluster gives you a 98.5% accuracy of CIRS3.
CIRS Tests:
Evaluations include assessments of proteomics (protein expression), neuroinflammation, transcriptomics (rna), immune dysregulation, hormonal imbalances and can be verified using secondary assessments including cardiopulmonary exercise testing, CNS volumetric programs, echocardiography, autonomic testing, biliary testing and more. There is not a lack of testing that exists for this, physicians just need to know what to test.
CIRS blood work usually includes:
- Hypermobility and +AGA and +ACLA
- Low MSH, high C4a, high TGF beta-1, high MMP9, HLA susceptibility
- Abnormal vWF (somewhat rare), abnormal VEGF, 80% of patients have MARCoNS
Other CIRS tests and common results:
- Depressed VO2 max and anaerobic threshold
- Elevated pulmonary artery pressure at rest/exercise
- Abnormal fingerprint on NeuroQuant
- Common incidence of gray matter nuclear atrophy
- More common incidence of interstitial lung disease and gastroparesis (anecdotal)
- Increase in abnormal ribosomal and nuclear encoded mitochondrial injury - can be monitored with blood work
VCS (Visual Contrast Sensitivity) Testing:
While this seems like a super strange way to test for biotoxin illness, VCS testing has been used for over 50 years in the air force to study toxins like heavy metal toxicity, hydrocarbon and petrochemical exposure. VCS testing was also used to help identify Pfiesteria toxicity in the 90’s. It’s a test that identifies whether or not you can see the contrast between gray and white lines, results are compared to controls. VCS results can show when you’ve had an exposure and should normalize afterwards. Failure of the test correlates with measured retinal capillary hypoperfusion to the neural rim of the optic nerve head.
There are a ton of examples of biotoxin illness impacting scores of people who are genetically susceptible.
How VCS Testing Works:
VCS looks at how well you identify contrast lines. Each orange diamond spot seen below measures a certain number of contrast lines, measured on the x access (called cycles per degree of visual arc). On the test these cycles will be shown to you at different angles (degrees). On the Y access it measures how much contrast you’re able to identify. The X access score correlates with how many lines you’re seeing and the Y access score identifies how much contrast you need in order to see the lines. The lower the score, the more contrast you need to see lines and the more impacted you are. This correlates with symptom number. Examples of VCS tests correlating with biotoxin illness are listed under Papers at the end of the doc.
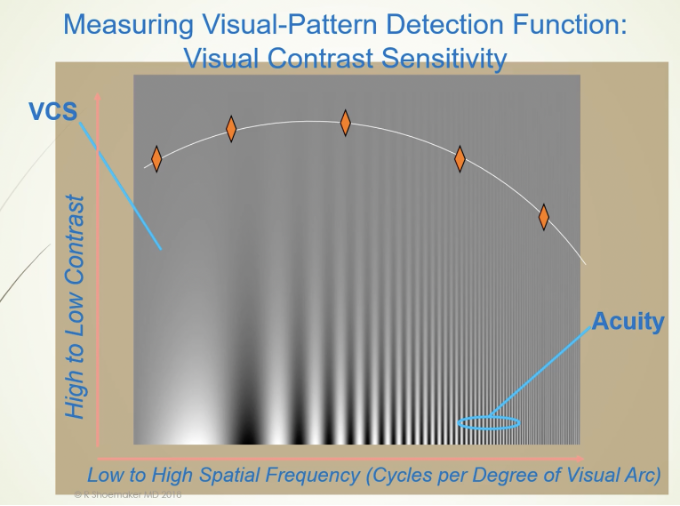
VCS Testing (looks like a total scam but it’s legitimate) (see Papers).
MARCoNS (Multiple Antibiotic Resistant Coagulase Negative Staphylococci):
CIRS: 80% of patients with CIRS are positive for MARCoNS. More common in patients with low MSH.
Function: Biofilms produced by MARCoNS, other bacteria, and/or yeast form a barrier to immune defenses and anti-infective therapies. Researchers suspect that bacterial biofilms may account for some cases of chronic nasal and sinus congestion and inflammation.19 MARCoNS release exotoxins that may damage MSH and thus impair its ability to coordinate dendritic cell responses within gut and respiratory mucous membrane compartments.20 MRCoNS also release hemolysins, which disrupt red blood cell and endothelial cell membranes, increasing the risk of coagulation abnormalities and anti-phospholipid antibody activity.4 When MARCoNS is plated, polycyclic ethers similar to a toxin produced by dinoflagellates (palytoxin - super toxic) appear.
Symptoms: Caused by living in a water damaged environment. Nasal and sinus congestion and inflammation. Contributes to feeling awful with CIRS
Testing: Nasopharyngeal culture ordered here.
Treatment: It used to be treated with BEG but due to antibiotic resistance it’s now treated with EDTA and silver. MARCoNS needs to be treated and eradicated before CIRS can be fixed. VIP (Vasoactive intestinal polypeptide) doesn’t work until MARCoNS is eradicated. It resides deep in the nasopharynx and can also cause jaw and tooth damage from cavitations in the mouth. EDTA plus silver is used 3x a day as a nasal spray generally for about 3-6 months. DO NOT take anti-fungal nasal sprays or treat candida systemically - it can breed further antibiotic resistance. Papers listed under papers.
NeuroQuant:
Doctors: https://www.cortechs.ai/locations/
CIRS causes edema in certain areas of the brain, and atrophy in others. NeuroQuant® is a software program approved by the FDA for measuring brain MRI volume from 2007. NeuroQuant® automatically identifies several MRI brain regions and measures the volume of each. These data are then compared to MRI data from normal control subjects. In addition to the NeuroQuant® standard report (which measures 11 brain regions but compares only 3 regions to normal controls) we have extended the utility of the test by identifying 15 brain regions, comparing all 15 to normal controls, and examining longitudinal change (obtaining 2 MRIs in the same patient, several months apart, and looking for progressive atrophy). Example NeuroQuant® extended report.5 Shoemaker has papers showing reversal of grey matter atrophy like that seen in dementia from VIP treatment… this is insane.6
- Results change over time with treatment (atrophy and brain edema can be fixed by CIRS treatment and VIP for 6 months)
- Can show a CIRS brain “fingerprint” and a post lyme “fingerprint”.7
- Warning: Atrophic nuclear atrophy is significantly worse particularly in patients over 40 if antifungals have been used
- Can cause an enlarged amygdala - stays the same with age. Enlargement seen with anxiety.
- Can cause an atrophied caudate - stays the same with age.
- Hippocampus - stays the same with age. Enlargement in PANS and atrophy in Alzheimer’s (possibly).
- Putamen - size decreases with age.
- Pallidum - size decreases with age.
- Thalamus - doesn’t change with age. Increase in size on the right side in Lyme, atrophy rules out Lyme disease.
- Mean cortical grey volume - size decreases with age.
- Lateral ventricle - size increases with age. Cortical grey determines the size of the symmetry of the lateral ventricle. With atrophied cortical grey - lateral ventricle size increases.
Testing: You need a requisition and you need to make sure the lab can do NeuroQuant, not all can provide this service.
Blood Markers:
(Skip everything other than Genes and go ahead to Treatment unless you really want to get into the details. If you want to get into the details the Definitions section can help). 4 of these blood markers need to be wonky (plus symptoms plus exposure plus genetic predisposition) to be diagnosed.
Genes/Genetic susceptibility:
95% of CIRS patients have a susceptible gene marker or markers. HLA DRB and DQ susceptible haplotypes. These are gene markers that correlate with imbalanced innate immune responses and/or defective adaptive immune responses to biotoxins.8
Chromosome 6 contains human leukocyte antigen alleles. HLA controls how antigen (pathogens) presenting cells identify antigens as foreign. Six of 54 HLA haplotypes are associated with CIRS. They’re found in roughly 24% of the population. To compare, 4 HLA haplotypes are associated with 95% of patients with chronic lyme disease (lyme disease that stays around after treatment is actually CIRS), those haplotypes are found in 22% of people who contract lyme. That’s why some lyme patients stay sick - they need CIRS treatment and lyme treatment.)
CIRS HLA Susceptible Haplotypes:
- 4-3-53 – has 12 subtypes DRB1- 0401, -0402 and -0404 are the worst, 3% incidence, the worst RA, malaria, autoimmune hepatitis. Have the highest C4a and TGF beta-1. 0401 is the worst.
- 11/12-3-52B – 1% incidence, tall, hypermobile, long arm span, good athletes. With free/unbound TGF β-1, they get “sicker quicker” upon exposure.
- 17-2-52 A, B, C and 7-2-53 haplotypes associated with celiac disease
- If a Lyme patient does not have the Lyme or multi-susceptible haplotypes there is a higher chance that he will respond to antibiotics alone.
- If the patient is not better with antibiotics and he has one of these haplotypes, he will need a biotoxin pathway approach. Taking antibiotics for prolonged periods alone will not fix these patients.
- Low risk mold HLA types are: 7-9-53; 12-7-52B; 9-9-53;
- No recognized significance types are: 8-3,4,6. 1-5,6,89
Testing: To test your susceptibility test HLA DR1, 3, 4, 5 and DQ through Quest or Labcorp (unfortunately not available in Canada).
alpha-MSH (Melanocyte Stimulating Hormone):
CIRS may cause: Reduced MSH level in 95% of CIRS patients. Normal Range: 35-81 pg/ml.
Function: MSH is a hormone marker of neuropeptide control of multiple functions including mucous membrane-based immune defenses, appetite, mood, circadian rhythms, pulmonary responses, blood-based immunocyte responses, gut tight junctions. Alpha-MSH binding to receptors in the brain and on white blood cells reduces inflammatory responses, including decreased production of pro-inflammatory cytokines.10,11,12 MSH is one of the most critically suppressed neuroregulatory peptide hormones in the dysregulation seen in CIRS patients.
Symptoms: Circadian rhythm disruption - sleep problems, leptin resistance (weight gain), fibromyalgia like pain (stabbing, aching, sensitivity to touch, etc.), controls tight junctions in the gut.
Testing: Quest and Labcorp normal ranges are off. The normal range is 35-81 pg/ml. Do not pay attention to the ranges provided by the labs, the actual peer reviewed scientific literature lists 35-81 pg/ml as the proper range for people. People with CIRS will generally have low MSH.
TGF beta-1:
CIRS may cause: Elevated TGF-beta 1 levels. Normal Range: <2380 pg/mL.
Function: TGF beta-1 is a cytokine and marker of an overactive immune system. TGF-beta 1 is a multifunctional cytokine that can inhibit the proliferation, differentiation, activation and effector functions of various immune cells (e.g. it’s in charge of sending T regulatory cells into tissue to reduce autoimmunity and reduce inflammation). TGF-beta 1 also does tumor suppression and promotes tolerance to allergens and self-antigens.13 TGF-beta 1 can also mediate pathology. It has been shown to promote immune evasion leading to chronic infections, and chronic elevations remodel various interstitial tissues resulting in fibrosis (if ROR is suppressed T regs turn into T-effector (cytotoxic) cells and cause tissue damage and fibrosis in kidneys, lungs, etc). People with HLA 11-3-52B usually have the highest markers for TGF-beta 1. TGF-beta 1 is also a marker used for long covid sufferers who have fibrosis as well (some studies show that long covid is CIRS).
Symptoms: Fibrosis in kidneys, lungs, skeletal muscle.14 Could look like thickened thigh muscles that won’t loosen up for example.
Testing: Normal Range: <2380 pg/mL.
Treatment: losartan, VIP
Complement C4a:
CIRS may cause: Elevated C4a levels (carnivore diet seems to lower this - paper coming soon). Normal Range: 0-650 ng/mL.
Function: C4a is an innate immune system activity marker/enzyme. C4a elevations represent an excessive innate immune response (complement system) to biotoxins. High C4a is also associated with cognitive deficits, restrictive lung disease, hypersensitivity pneumonitis, and multisystem, multi-symptom illness from chronic fatigue.15 Based on Shoemaker’s analysis of biomarkers, targeting the cause of over-expressed MASP 2 activity could be the most beneficial way of intervening to keep CIRS signs and symptoms under control even in the face of re-exposures. Re-exposure to biotoxins raises levels in 4 hours, and re-exposure to Lyme brings a rise in 12 hours. It appears as if this can be kept lower by the meat diet as well (anecdotal from a number of people’s markers dropping with diet). Increases lactate contributing to muscle soreness. High C4a levels are also seen in lupus and Lyme disease.16
Testing: Shoemaker says not to use LabCorp to test (use Quest) because Labcorp adds futhan to the vials to help with freezing. I’m not sure how that matters but he says don’t use labcorp. You can do a pretty easy test using a tic tac toe test on skin to see if people get hyper dermatographia. More info under Papers. Normal Range: 0-650 ng/mL.
MMP-9 (Matrix Metalloproteinase-9):
CIRS may cause: Elevated MMP-9 level. Normal range: 85-332 ng/ml; 28.14-109.89 nmol/l.
Function: MMP-9 is an innate immune system activity marker/enzyme. In biotoxin-related illnesses, MMP-9 is a gelatinase enzyme that tunnels through endothelial and matrix tissue barriers, delivering inflammatory markers out of the blood.
Symptoms: Higher levels of MMP-9 have been associated with increased tumor invasiveness, and with increased permeability in the blood-brain barrier.17,18,19 MMP-9 is a marker of inflammation, tissue remodeling, wound healing, and mobilization of tissue-bound growth factors and cytokines20. Increases after 60 hours of exposure.
Intensification reactions when starting treatment due to rising MMP-9 are common in people with Lyme or MARCoNS. The initial binder treatment for CIRS - cholestyramine (CSM) - can worsen these reactions if the binder is introduced too quickly or without fish oil (see CSM for more details).
Testing: Blood needs to be taken in chilled vials by the lab, and spun immediately or levels aren’t measured properly. Sent frozen for measurement. MMP-9 can double in 30 minutes at room temperature. Normal range: 85-332 ng/ml; 28.14-109.89 nmol/l.
Treatment: MMP-9 can be lowered by high dose omega-3’s and EPA and DHA 2.4g EPA and 1.8g DHA. For people on the lion diet - wild salmon is fairly well tolerated if omega’s are intolerable, canned sardines/mackerel would be better but higher in histamine levels.
Previous treatment: The rx Actos was used effectively to lower MMP-9 but now has a black box label that Shoemaker thinks is unwarranted.
ADH/Osmolality (Vasopressin):
CIRS may cause: Reduced ADH (generally but not always) and elevated osmolality levels. Or just levels get weird in either direction. High and high, low and low, high and low or low and high. ADH Normal Range: 1.0-4.7 pg/mL. Normal Range: 280-300 mOsmol/kg. Osmolality is abnormal at levels of >295 or <275
ADH is abnormal at levels of <1.3 or >8
Values are also abnormal when ADH is <2.3 with an Osmolality of 292-295
Or when ADH >4.0 with an Osmolality of 275-278
Function: ADH is the antidiuretic hormone (vasopressin) which stimulates cells in renal tubules to reabsorb free water in response to rising osmolality (saltiness) of blood. It’s a marker of disrupted MSH function. Reduced hypothalamic output of ADH in response to hyperosmolarity (vasopressin is known to regulate blood pressure, blood osmolality, and blood volume) is associated with reduced VEGF production in response to low microcirculatory oxygen levels.21 Low ADH receptor function is likely to result in lower ADH signaling in the amygdala.
Symptoms: Blood pressure issues - can cause POTS (blacking out when standing up) and headaches and migraines. Thirst, frequent urination, bed wetting in kids. Static shocks too from more salt on the skin. Weird eh? Genetically associated decreases in ADH receptor production are associated with autistic behaviors as well.22
Testing: ADH Normal Range: 1.0-4.7 pg/mL. Normal Range: 280-300 mOsmol/kg.
Treatment: Can be treated with DDAVP (0.2mg QOHS). Monitor for low sodium (increase salt while taking this). One dose for 5 days at night. Monitor electrolytes and weight.
ACTH (Adrenocorticotropic Hormone)/Cortisol:
CIRS may cause: high or low ACTH/Cortisol.
Normal Range: 8-37 pg/mL; 1.76 – 8.14pmol/L
Function: ACTH is a hormone made by the pituitary gland, a small gland at the base of the brain. ACTH controls the production of another hormone called cortisol. Cortisol is made by the adrenal glands, two small glands located above the kidneys. Cortisol plays an important role in helping you to: Respond to stress.23
Symptoms: NOT caused by adrenal insufficiency (Addison’s) or Cushing’s but may be misdiagnosed as that. Inability to handle stress, fatigue, insomnia.
Avoid: Do not take steroids to fix this (prednisone, etc.)
- Short topical is okay
- Joint injections are okay
- Medrol dose packs are not good
- Prednisone is not good
- Steroids are more difficult for people with low MSH to come off of
Testing: 8-37 pg/mL; 1.76 – 8.14pmol/L
Treatment: CIRS protocol (not adrenal insufficiency)
Leptin:
CIRS may cause: high leptin levels. Leptin normal range: men 0.5-13.8 ng/ml; women 1.1-27.5 ng/ml. Range varies with BMI.
Function: Leptin is a peptide hormone synthesized by white adipose tissue. High levels of leptin increase the amount of fat stored in the body, causing weight gain. In biotoxin-related illness, cytokines attach to leptin receptors in the hypothalamus, interfering with leptin signaling and creating leptin resistance. Weight gain due to leptin resistance is common in CIRS patients (this does seem to be helped by diet). Also in the hypothalamus, leptin activates pro-opio-melanocortin (POMC) neurons, which release alpha melanocyte stimulating hormone (MSH). Because of leptin-receptor damage, POMC pathway communication is impaired and MSH production is reduced, leading to the loss of hormonal regulation.
Symptoms: Rises on the second day of exposure. Increase in hunger. Weight gain. Weight gain even with the same amount of calories.
Testing: Leptin normal range: men 0.5-13.8 ng/ml; women 1.1-27.5 ng/ml.
Treatment: CIRS treatment. The lion diet can also decrease hunger and help with weight loss even with CIRS.
VEGF (Vascular Endothelial Growth Factor):
CIRS may cause: Reduced VEGF level in ⅓, elevated level in ⅓ and normal in ⅓ of patients. Ignore high levels unless levels are above 600 - and then an octreotide scan looking for a APUDoma tumor is warranted. Normal Range: 31-86 pg/mL.
Function: a marker of capillary hypoperfusion (reduced blood flow). Increases new blood vessel formation and increases oxygen delivery. Early in CIRS, VEGF can run high, a sign that it is trying to help compensate for low oxygen delivery to tissues. A low level indicates VEGF burnout. Capillary hypoperfusion stimulates VEGF, rising VEGF stimulates TGF beta-1, TGF beta-1 suppressed VEGF,
Symptoms: Possible muscle weakness. A low level of skeletal muscle VEGF is associated with decreased muscle endurance.24 Can correlate with low VO2 max. Rises on day 1 and falls on day 3 of exposure after TGF beta-1 rises.
Testing: Look at plasma VEGF not serum. Normal Range: 31-86 pg/mL.
Treatment: Omegas (like treatment for MMP9). High dose fish oil (2.4g/EPA and 1.8g DHA using a 875/67 enteric coated capsule. If there are no responses, use VIP.
Anti-Gliadin Antibodies:
CIRS may cause: Elevated anti-gliadin antibodies (markers of leaky gut and increased risk for autoimmune reactivity).
Function: The antibodies bind to gliadins. Gliadins are indigestible fragments of gluten. In cases where intestinal hyperpermeability is present (more likely with a low MSH level), one of two forms of gluten reactivity may present: non-celiac gluten sensitivity (a milder but still problematic form of reactivity in those who are not genetically prone to celiac disease), and celiac disease.25
Symptoms: Gut distress, bleeding, bloating, diarrhea. CIRS can look like Celiac Disease.
Treatment: Go gluten free. This is avoidable if you just don’t eat gluten - gluten should be avoided in my opinion anyway, there are a ton of health issues associated with consumption of gluten that are not CIRS related so this won’t be an issue if you’re not eating it anyway, however low MSH can causes loose tight junctions which does make gluten (and a ton of other foods) an issue. Hence the lion diet as combined therapy for CIRS.
VIP (vasoactive intestinal peptide):
CIRS may cause: Reduced VIP level. Normal Range: 23-53 pg/mL
Function: a marker of blood flow regulation and distribution. Low levels are associated with capillary hypoperfusion and abnormal pulmonary artery pressure at rest or in response to exercise. VIP helps determine which antigens the immune system will tolerate and is an important down-regulator of inflammation.26 Vasoactive Intestinal peptide (VIP) is a neuro-regulatory hormone produced in the suprachiasmatic nucleus of the hypothalamus, gut and pancreas. VIP has been used as an alternative treatment for autoimmune disease. It down-regulates cytokines, inhibits the production of TGF beta 1 and modulates T regulatory cells27,28.
Symptoms: Heart palpitations. Inability to exercise without shortness of breath. Arthritis, joint degeneration.
Testing: Normal Range: 23-53 pg/mL
Treatment: VIP compounded - Hopkinton Drug 800-439-441 (more under Treatment).
vWF (von Willebrand Syndrome):
CIRS may cause: von Willebrand Syndrome. Values will be high or low. Rare in general population (20/100 000) - not as rare in CIRS (35/1300).
Function: Basically this stops endothelial cells from going from monomer to polymer and stopping bleeding.
Symptoms: Increased bruising, can cause nose bleeds that won’t stop basically. Rise of factor 8 on day one of exposure, recovery on day 3 but on day 3 fall of ristocetin associated co-factor and vWF antigen and nose bleeds day 4.
Testing: Quest comprehensive panel (include multimers).
Treatment: Can be treated with DDAVP (one tablet can stop bleeding).
Vitamin D:
CIRS may cause: reduced levels of Vitamin D.
Plasminogen activator inhibitor-1 (PAI-1):
CIRS may cause: reduced levels of PAI-1.
Function: Plasminogen activator inhibitor-1 (PAI-1) is a serine protease inhibitor secreted by the endothelial layer of blood vessels and adipose tissue. It inhibits fibrinolysis, increases clotting and causes increased risk for thrombosis. When MMP-9 combines with PAI-1, it can facilitate oxidized LDL to move through blood vessel walls. This brings inflammatory elements into the sub-intimal space which can cause fibrosis of connective tissue and atherosclerosis.29
Test: Normal Range: 5-40 mg/l
Pulmonary Hypertension:
CIRS can cause: elevated levels.
Function: High blood pressure in the blood vessels leading from the heart to the lungs.
Symptoms: Commonly misdiagnosed as asthma. Can cause heart palpitations.
Treatment: when lipase is normal, VCS is normal, MARCoNS is absent, HERTMI-2 <11, GGTP normal, use 1 spray of VIP QID intranasally (increase over one week) for 30 days. If PASP is not decreasing, increase VIP to 2 QID.
VO2 Max:
CIRS can cause: reduced VO2 max
Function: VO2 max measures how much oxygen (usually in milliliters) you breathe in while exercising as hard as you can. The more oxygen you inhale, the more energy your body can use. Higher VO2 max usually means better physical fitness. Low VO2 max is common in chronic fatigue. Not enough oxygen getting to mitochondria reduces how much ATP they can make.
Symptoms: chronic fatigue, shortness of breath, asthma like symptoms, heart palpitations, post exercise cognitive dysfunction.If you do more one day (mow the lawn) and symptoms are worse following for a few days. Inability to perform exercises for more than 1-2 minutes. 5% efficiency at burning glucose for CIRS patients (reasons for a ketogenic diet?).
Testing: Measured by a pulmonary lab
- CPET - cardiopulmonary exercise testing
- Valid indicator of functional capacity (O2 consumption in ml/kg/minute)
- Do not do it on consecutive days if fatigued
- Anaerobic threshold is usually low in CIRS
Treatment: Symptoms theoretically could be reduced by high protein high fat ketogenic zero carb diet (lion diet). Anaerobic exercise daily (very slow just what’s tolerated max 45 minutes per day) can help.
POTS and PANS:
Postural Orthostatic Tachychardia Syndrome
Symptoms: blacking out when standing up and low blood pressure. Causes excessively reduced volume of blood returns to the heart after an individual stands up from a lying down position.30
Pediatric Acute-Onset Neuropsychiatric Syndrome
Symptoms: sudden psychiatric symptoms in kids.31 NeuroQuant shows hippocampal enlargement.
Testing: abnormality when testing adh/osmolality, elevated PASP.
Treatment: CIRS treatment. When MSH markers normalize, and VCS tests are negative, no MARCoNS and the environment is clean (HERTSMI score is good) symptoms disappear. If not, use DDAVP and then VIP. (For PANS if psych symptoms aren’t severe, a month of CSM seems to do the trick plus removal from the water damaged environment).
GENIE:
Does transcriptomics testing to monitor. Hypometabolism (caused by CIRS and other illnesses) includes pathologic suppression of both ribosomal and nuclear-encoded mitochondrial genes. Actual mitochondrial genes still resident in mitochondria number 37; the other 1000 or so are in our own nuclear DNA. Hypometabolism shows us the dominant role of differential gene activation in pathogenesis and perpetuation of chronic fatiguing illnesses.
Treatment of hypometabolism with our published, peer-reviewed protocols shows sequential resolution of gene suppression/activation. For the first time we can now track the pathological basis of chronic fatigue and critical inflammatory elements throughout treatment.
Testing (test ordered here by you, about $700). Instructions under GENIE under Treatment.
Treatment
Read the Treatment page linked above, it's much more in-depth than what I have here.
What To Do and NOT To Do:
- Do NOT take antifungals. Antifungals can breed antibiotic resistance in bacteria in as little as one month. Doctors treating MARCoNS with anti-fungal nasal sprays had patients with more resistance to treatments than other patients, within a month. Do not take them as a spray or systemically. There’s also evidence it can seriously badly contribute to grey matter atrophy. If you don't get better from CIRS treatment - maybe trying an antifungal is worth a shot to see if it addresses an actual infection but those are rare.
- Use glutathione carefully - glutathione can increase levels of gliotoxins and make you feel awful.32 However glutathione levels are also seriously depleted with mold exposure so supplementation can help that. I'd start slow with oral glutathione and work your way up to IV drips then pushes if tolerated. Just don't start at pushes if you're quite sick, they made me feel worse.
- Do NOT do the treatment out of order. Start from the bottom of the pyramid and work your way up (combining treatment with diet).
- Make sure you address your diet at the same time.
1. Removal From Exposure:
Making Sure You’re Not Exposed: Test Your Living Area
This is the most important thing you can do. You will not heal if you’re being re-exposed even if you’re treating CIRS. This is why people do not heal. Even with treatment, exposure will cause symptoms. Everywhere you “live” needs to be tested. That’s your house, school, and office if you don’t work from home. If you’re experiencing symptoms (or your child is), everyone who lives in the house needs to test where they spend time as well, as toxins can be brought home from infected buildings. I put together a list of easily implementable cleaning techniques and products under FAQ! Check these out, that should help reduce exposure to these biotoxins quickly.
Shoemaker has shown that 95% of symptoms come back if re-exposed for 8 hours per day for 3 days by doing re-exposure tests on treated patients.
ERMI/HERTSMI-2 testing for molds:
Overview and availability of tests
The ERMI tests more strains of molds, the HERTSMI-2 score can be derived from the information on the ERMI test to give you a score of the worst molds for your health.
Scores: You want an ERMI under 2 or even under 1 for very sick people, and a HERTSMI-2 under 11. Note: I’ve been staying in a hotel with an ERMI of 2 and a HERTSMI-2 of 4 and still feel like garbage (although much better than the Florida house that scored 20). Technically the ERMI score of 0 is where the 50th percentile house is in the US in regard to mold so I don’t really understand how 0 is good enough for CIRS. But that is what Shoemaker has shown is good enough for CIRS.
Mold hides behind walls and isn’t always visible, but if it is visible it’ll be in commonly water damaged areas that can include:
- Basements
- Attics
- Sinks (underneath and in the sink)
- Washing machines (particularly front loading - wipe these with vinegar each time they’re used and dry thoroughly - replace the rubber ring if it’s moldy ASAP)
- Shower grout (bathtubs are safer)
- Anywhere with any water damage (bubbling paint)
- Anywhere showing rust
- Around windows
- Around doors
- HVACs particularly in high humidity areas
Ineffective Testing:
Regular mold testers do not know what they’re doing. Calling up anyone will not work. They’ll test the air quality by testing spore count in the air. 0.2% of particulate matter is actual whole spores in air. Everything else is fragments or bacteria. Testing needs to be done extensively, should take a number of hours, and ideally the testers test behind walls in a few areas.
Companies:
The only company I trust is MoldFinders and they’re expensive and are booked 6 weeks out. They’re the best, but ERMI and HERTSMI-2 tests will give you very good answers if done properly, and can have turn around time of 24 hours. You can do this testing yourself, but don’t fix the mold yourself - especially if you’re sick. Remediation is complicated but doable.
Endotoxin testing: ERMI and HERTSMI-2 test molds. Endotoxin testing is also important and can be tested but ERMI and HERSTMI-2 will give you enough information and endotoxins and actinomycetes toxins don’t generally test high if the ERMI and HERTSMI-2 are low. Envirobiomics offers an ERMI with endotoxin testing as well.
2. Binders:
Cholestyramine (CSM) (or Welchol) (prescription):
CSM is a resin, originally used to treat high cholesterol (another reason to increase fat with diet while using this). It’s also used to help with Ulcerative Colitis, IBD, IBS, etc. CSM has worked insanely well for me. It was rough at first - I had intensification reactions (worsening of symptoms) with the full dose. Symptoms for me would feel better almost immediately upon ingestion and then worse while the CSM traveled through my digestive system. The first two weeks were pretty up and down. Intensification reactions are common (particularly in lyme and MARCoNS patients). They can be reduced with EPA/DHA and omega 3 supplementation (or if those are not tolerated, start with a low dose of CSM and titrate up and make sure you have bowel movements (BMs) every day - use magnesium citrate if needed. Getting the toxins out of you is the goal so BM’s are mandatory daily. Intensification symptoms (your normal biotoxin symptoms flaring up) seem to happen when the CSM moves into the digestive tract re-exposing you to the toxins. Once you have a BM you feel better quite quickly. (Starting CSM and experiencing intensification reactions usually includes a fall in the VCS score (in column D and E) and a rise in MMP-9).
- Get the compounded version (unflavored pure resin)
- CSM and Welchol do successfully reduce all symptoms, stop secretory diarrhea, and help improve VCS scores.
- Treatment for children with CIRS is only complete removal from exposures and a binder!
- Side note: Shoemaker never found toxins in stool of patients using CSM - weird. Binding theory hasn’t been proven by finding toxins in stool but it does work to reduce VCS scores and definitely binds bile (where toxins are put from the body).
- Children tolerate this better
- CSM needs to be taken 30 minutes before eating or two hours after to avoid binding nutrients - adding fat 30 minutes after eating helps
- Welchol needs to be taken with food
For people with food and chemical intolerance - diluted VIP may be used before CSM so that treatment is tolerated.
Other Binders:
- I found activated charcoal (not prescription) to help my secretory diarrhea and stomach upset before I started CSM. There’s no peer-reviewed evidence that activated charcoal, bentonite clay, chlorella, or other binders help improve VCS scores, but anecdotally people do say activated charcoal and bentonite clay can help. They are not as effective as CSM by far. There are also animal studies using charcoal to bind toxins successfully.33
Also 2. Fish Oil:
People with Lyme or MARCoNS (or toxin overload) can have intensification reactions when starting CSM/Welchol. High dose Omega 3 treatment is highly recommended to start before CSM or Welchol or at least at the same time.
Also 2. Diet:
An all meat diet is not part of the Shoemaker protocol (he suggests a low amylose diet) however I think it’s basically necessary to speed up recovery from CIRS and deal with current symptoms. It’s anecdotally VERY effective (from 10 000 people).
Diet can be extremely helpful for a number of reasons. Many foods contain biotoxins and mold. Some are worse than others and those include:
- Sugar and starchy foods (feed candida and other biotoxins in the gut)
- Dried foods (higher in mold)
- Beans, coffee, chocolate (higher in mold), soy
- Grains (higher in mold) including corn. Particularly gluten containing grains
- Alcohol
- Vinegar
If CIRS causes damage to the gastrointestinal tract and a hyperactive immune system that then reacts to everything (animals, environmental allergens, soaps, detergents, scents, VOC’s, chemicals, even EMF’s for some seriously unfortunate people) it can/will cause a reaction to foods as well, including foods with molds on them. Removing plant foods and even some specific meats and all dairy can reduce the amount of exposure to biotoxins you’re consuming, shouldn’t trigger an immune response as easily, can moderate hunger due to leptin damage, reduces the amount of food that could be leaking into the blood due to a damaged gut provoking an immune response, and doesn’t feed current infections in the gut (such as Candida overgrowths). An all meat diet does this and can be hugely beneficial to patients - an all ruminant meat diet also reduces exposure to toxins in animals that are normally inhaling these biotoxins (pigs and chickens from where they’re kept).
Another potential reason: CIRS patients can’t use glucose effectively. Their cells can be reduced to 5% efficacy for glucose metabolization (especially with chronic fatigue) (Shoemaker). Why not sidestep the entire problem and feed cells ketones? Researchers are seeing if CIRS impacts ketone utilization as well - if so, ketones wouldn’t matter as much. Either way, diet isn’t enough to solve the root problem but it can help survive it.
Shoemaker suggests (directly from survivingmold.com):
You should not: Consume metabolic poisons like sugar, aspartame, Sucralose, monosodium glutamate (MSG), pesticides and insecticides (used on conventional produce), GMOs, antibiotics, growth hormones, and unnatural diets (used on conventional farm animals), toxic inflammatory oils like soy and canola.
You should: Eat foods that are as natural, healthy and organic as possible. Use only organic butter, coconut oil or olive oil.
You should not: Over consume carbohydrates (breads, rice, pastas, starchy vegetables) this will increase your insulin levels. High insulin contributes to every chronic degenerative disease by increasing inflammation in your body. High insulin also changes your androgens (like testosterone and DHEA) into estrogens by stimulating your aromatase enzyme
Another potential reason to use the lion diet after exposure to biotoxins is to use mycotoxin urine tests. Generally these are useless because your diet can impact the amount of mycotoxins you have in urine (you could be completely healthy but have a high level of mycotoxins in your urine if you’re drinking moldy coffee, etc.) but that’s not a factor on an all meat diet. Then there’s another way to measure mycotoxin levels that wouldn’t be available to people with varied diets. In theory.
3. MARCoNS
MARCoNS needs to be eradicated in order to use VIP. EDTA spray plus silver spray 2 sprays 3x a day for 3-6 months kills it. Start 30 days after binders. Gene suppression due to MARCoNS seems to get a lot better after 2 weeks. Shoemaker suggests continuing this to ward off future infections for people with low MSH.
4. Possibly some of these are necessary:
DDAVP:
- Peptide, not necessary for everyone
- Used for nose bleeds that won’t stop - in tablet form
- Macrodoses for pulmonary hypotension
- Teaching VIP video ($30)
Actos:
- Used to be used to correct MMP-9 levels
- Now has a black box warning that Shoemaker thinks is unwarranted and is rarely used
Losartan:
- Corrects TGF-beta if necessary.34
- Blood pressure needs to be 130/85 at least (causes low blood pressure).
- Losartan has an active metabolite called EXP3179 that lowers TGF-beta 1.
DHEA:
- Androgens usually fix themselves - don’t add in testosterone.
- 3x a day for a week - measure estrone and dhea at baseline - if androgens go down and estrogen goes up that means estrogen is working on the extra dhea.
- Do not add in an aromatase inhibitor (like clomid) in low MSH patients - it’ll make things worse
5. VIP (Vasoactive intestinal polypeptide):
Before VIP can be taken the patient needs to have a normal VCS (normalizes after no exposure), normal nasal culture (no MARCoNS), normal HERTSMI-2 or ERMI (living and working areas with no exposure), normal lipase and normal GGTP.
Treatment: Compounded VIP intranasal 50 mcg/dose of 0.1ml. Normal dose is 4x a day. 120 doses/month = 12ml. Use microdoses for chemical and food sensitivities and for serious illness (1/100th or even 1/1000th of dose). Test 1 spray dose in the office (50mcg/100mcl) by measuring TGF beta-1. If it rises more than 33%, the patient is still exposed to biotoxins somewhere. After several months VIP can be cut down to 2x per day.
- Monitor treatment with Nanostring (measures gene expression changes during treatment)
With new exposures CIRS symptoms can come back and the entire thing might need to be restarted so not living in exposure is beyond key unless you want to do this for the rest of your life.
For people with food and chemical intolerance - diluted VIP (1/100th or 1/1000th) may be used before CSM so that treatment is tolerated - for people with multiple chemical sensitivities and food sensitivities this might be warranted.
Definitions:
Gene Definitions:
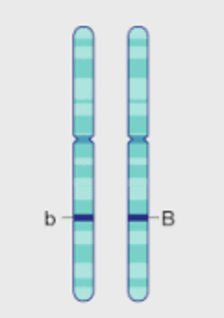
Alleles:
An allele is a specific form of a gene organized by different variations of nucleotides.
(b and B are different alleles on a chromosome). You get different alleles from your mom and your dad. Alleles are different variations of genes (e.g pink vs white flower petals). Or in CIRS - predisposition to an HLA-DR MHC II receptor that doesn’t identify biotoxins properly vs. one that does.
Chromosome:
A bunch of DNA. Or, from Oxford: threadlike structure of nucleic acids and protein found in the nucleus of most living cells, carrying genetic information in the form of genes.
Gene:
A gene is a segment of DNA that determines a certain trait. An allele is a specific form of the gene organized by different variations of nucleotides.
Haplotypes:
A haplotype is a group of alleles that are inherited together from a single parent. Recombinant versions are rare because they’re usually located closely on a chromosome.
HLA:
Human leukocyte antigen genes. Everyone has these, not everyone has the alleles that predispose them to CIRS. They code for cell surface antigen receptors. HLA refers to the Human Leukocyte Antigen genes on chromosome 6. HLA’s are found on the surface of nearly every cell in the human body. They provide instructions for making a group of related proteins known as the HLA complex which helps the immune system distinguish between the body’s own proteins and proteins made by foreign invaders such as bacteria, viruses, and fungi. This gene encodes for proteins that present foreign antigens to immune cells for removal. The HLA tests determine one's susceptibility to CIRS plus many other diseases.35
Immune System Definitions:
HLA-DR/DQ:
HLA DR/DQ encoded proteins are found on antigen presenting cells such as macrophages, B cells and dendritic cells. They present foreign cells from outside the cell to naive T lymphocytes. The T lymphocytes eliminate the antigen and transfer to B lymphocytes the ability to identify the antigen for removal. The structures of the HLA molecules are critical to the initial peptide/antigen recognition. The alleles most important for chronic illness expression include DRB1, DQ, DRB3, DRB4, and DRB5.36
HLA-DR is a type of MHC class II cell surface receptor encoded by the human leukocyte antigen complex on chromosome 6 region 6p21.31. The main function of HLA-DR is to present antigens from APC’s to the adaptive immune system (T cells) to elicit or suppress T helper cell responses that eventually lead to the production of antibodies against the same peptide antigen.
Antibody steps with HLA:
- Antigen detection
- Antibody formation
- Internalization of receptor and antigen
- Acidification of phagoendosome
- Send that to the ER and create a phagoendolysosome
- Add HLA DR in ER to dendritic cells
- Present to naive T cell and to B cell
MHC class I:
This is on the membrane of every nucleated cell. It presents an antigen if it’s infected with a virus or cancer. Killed by CD8+ T cells (cytotoxic).
MHC class II cell surface receptor:
The major histocompatibility class II cell surface receptor is one of the key cell surface molecules expressed on antigen presenting cells (monocytes, B cells, macrophages and dendritic cells), responsible for antigen presentation to CD4+ to T (effector) cells and initiation of the inflammatory cascade during infection as well as differentiation into effector or memory cell mode.
Peptide:
Two or more amino acids make a peptide. Polypeptides form proteins.
Antigen:
Antibody generating. Anything that can cause an immune response such as whole pathogens (bacteria, viruses, fungi), smaller proteins that pathogens express or parts of pathogens. Food that escapes from a damaged gastrointestinal tract can also become antigens.
Antibody:
A protein on the membrane of naive B cells (or can be free floating) that bind to antigens. Antibodies are created on the membrane of memory B cells and are also released to float around from B Cells/plasma cells to bind to specific antigens.
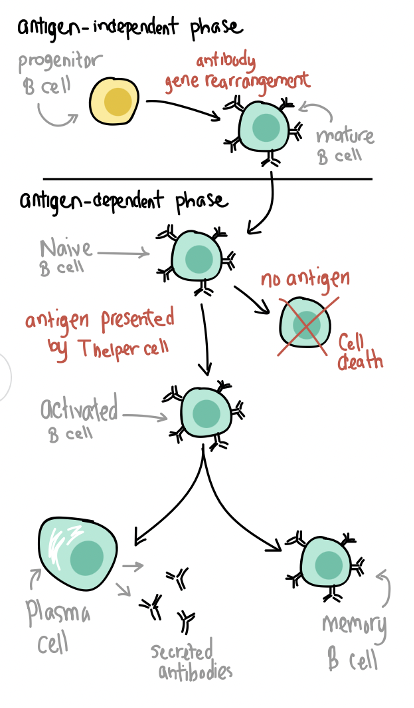
B cells:
Type of lymphocyte formed in the bone marrow from stem cells that produces antibodies to fight infection and present antigens to T cells. Starts with a naive B cell with antibodies of all shapes on its membrane. When an antigen is presented to a B cell from the innate immune system the B cell transforms into a memory B cell or a plasma cell. Plasma cells create more antibodies to bind more of that specific antigen for removal out of the body.
T cells:
A type of lymphocyte formed from bone marrow stem cells. They move to the thymus and mature and express T cell receptors and other receptors called either CD4+ (helper T cell) and CD8+ receptors (cytotoxic) depending on the T cell. They only recognize antigens that are bound to MHC1 and MCH2 on antigen-presenting cells (APC’s) like B cells, macrophages and dendritic cells, they don’t recognize free antigens like B cells. They also destroy cells that are infected. T cells also produce cytokines.
(Khan Academy)
Innate immune system:
Innate immunity is the first line of your body’s defense. It’s made up of different components that include physical barriers (tight junctions in the skin, epithelial and mucous membrane surfaces, mucus itself); anatomical barriers; epithelial and phagocytic cell enzymes (i.e., lysozyme), phagocytes (i.e., neutrophils, monocytes, macrophages), inflammation-related serum proteins (e.g., complement, C-reactive protein, lectins such as mannose-binding lectin, and ficolins); surface and phagocyte granule antimicrobial peptides (e.g., defensins, cathelicidin, etc.); cell receptors that sense microorganisms and signal a defensive response (e.g., Toll-like receptors); and cells that release cytokines and inflammatory mediators (i.e., macrophages, mast cells, natural-killer cells). Once the interaction host-invader pathogen enters, a signaling cascade is initiated which enhances the immune response and activates specific mechanisms. This natural immune response is designed to: a) prevent infection, b) eliminate invader pathogens, and c) stimulate the acquired immune response.37
Adaptive immune system:
If the innate immune system isn’t enough, the adaptive immune system is activated. Made of B and T cells. Adaptive immune responses are carried out by white blood cells called lymphocytes. There are two broad classes of such responses—antibody responses and cell-mediated immune responses, and they are carried out by different classes of lymphocytes, called B cells and T cells. In antibody responses, B cells are activated to secrete antibodies, which are proteins called immunoglobulins. The antibodies circulate in the bloodstream and permeate the other body fluids, where they bind specifically to the foreign antigen that stimulated their production. Binding of antibodies inactivates viruses and microbial toxins (such as tetanus toxin or diphtheria toxin) by blocking their ability to bind to receptors on host cells. Antibody binding also marks invading pathogens for destruction, mainly by making it easier for phagocytic cells of the innate immune system to ingest them.38
Adaptive immunity involves the destruction of foreign pathogens and presentation of their peptide remains to T cells to begin the process of antibody production by B cells, and NK cells and cytotoxic T cells. The T cells teach the B cells to recognize and respond to invading toxins so that, in the future, if re-exposed, antibodies produced by the B cells can mount an appropriate antibody response.
CIRS: In biotoxin illness, due to specific genetic HLA susceptibilities, the adaptive system cannot see the biotoxins presented to them by the innate system and thus cannot produce antibodies to neutralize them. The toxin isn’t recognized as foreign. These toxins have a unique structure called “ionophores” that prevent them being metabolized or excreted. The innate immune system continues to create inflammatory cytokines, leading to dysregulation of multiple systems and thus the CIRS diagnosis. Patients with CIRS have dysfunction of T reg cells which are converted into pathogenic T lymphocytes via the inflammatory cytokine TGF beta-1.
Complement system:
Complement is a system of plasma proteins that can be activated directly by pathogens or indirectly by pathogen-bound antibodies, leading to a cascade of reactions that occurs on the surface of pathogens and generates active components with various effector functions.39
Lymphocyte:
A type of white blood cell (B or T cell, NK cells). Natural killer cells recognize general signals of immune stress such as inflammation. B and T cells recognize antigens via B cell and T cell receptors. B cells also recognize free, unprocessed antigens. T cells recognize antigens within a complex of cell surface proteins called the major histocompatibility complex (MHC) on the surface of antigen-presenting cells.
Cytokines:
molecules that are used for cell-to-cell communication or cell signaling. Cytokines can communicate with nearby cells or distant cells to initiate an immune response. They also trigger cell movement to a specific area of the body.
Chemokines:
a type of cytokine that is released by infected cells in order to initiate an immune response or alert the neighboring cells of a threat.
Biotoxins:
any living organism or fragment of organism that triggers the innate immune response.
Current CIRS biotoxins:
Beta glucans, mannans, spirocyclic drimanes, actinomycetes, hyphal fragments, cell wall fragments, endotoxins, ribotoxins, MVOC’s, mycotoxins, hemolysins, proteinases, gram + and - bacteria, particulates, conidia, ribosomal inhibitory proteins. 80% of exposure happens in WDB.
Blood brain barrier (BBB):
Endothelial cells and tight junctions make up the blood brain barrier. High levels of MMP-9 can increase tight junction permeability in the gut and BBB. VEGF can also breach the BBB.
Capillary hypoperfusion:
Reduced blood flow.
PASP (pulmonary artery systolic pressure):
A normal pulmonary artery systolic pressure is less than 25 mmHg. Between 40 and 50 mmHg is considered a mild elevation. Anything greater than 50 mmHg is considered moderate elevation, and greater than 60 is considered severe.
TR (tricuspid regurgitation):
a type of heart valve disease that occurs when the valve's flaps (cusps or leaflets) do not close properly.
TRPV:
Transient receptor potential channels, of the vanilloid subtype (TRPV), act as sensory mediators, being activated by endogenous ligands, heat, mechanical and osmotic stress. Within the vasculature, TRPV channels are expressed in smooth muscle cells, endothelial cells, as well as in perivascular nerves.40 Impacted by biotoxins (like ciguatera).
Genetics:
The study of genes. (DNA structure, gene sequence, SNP’s, etc.)
Genomics/Transcriptomics:
The study of RNA molecules in a cell. RNA is copied from pieces of DNA and contains information to make proteins and perform other important functions in the cell (definition from the national cancer institute). Transcriptomics can show you how gene expression changes in different organisms. The genomics investigation of CIRS is focused on the expression of genes, or transcriptomics. Our research has identified nearly 2,000 statistically significant, differentially expressed genes in the average CIRS patient before they begin CIRS treatment. These abnormalities are dominated by genes involved in ribosomal protein and mitochondrial activity, resulting in a hypo metabolic cellular state. Additionally, many patients exhibit abnormalities in T cell receptors, insulin signaling, coagulation and various CD markers. We also looked at micro RNAs and have identified that Let7 and MIR23 family members contribute to CIRS pathology.41
Proteomics:
The study of the structure and function of proteins, including the way they work and interact with each other inside cells (from the national cancer institute). (Can be seen on lab tests). Many irregularities in protein expression have now been identified in patients with CIRS, dominated by (1) lack of regulation of host inflammatory response as evidenced by deficiency of alpha melanocyte stimulating hormone (MSH) and/or vasoactive intestinal polypeptide (VIP); (2) presence of more than one of Th1 responses (pro-inflammatory); Th2 responses (anti-inflammatory); Th17 responses (tied to transforming growth factor beta-1 (TGFβ-1)); coagulation abnormalities, especially abnormalities in von Willebrand’s profile; activation of complement split products; activation of elements under regulation of hypoxia inducible factor including vascular endothelia growth factor (VEGF) and erythropoietin; abnormal regulation of ACTH responses to cortisol and ADH responses to osmolality.42
Metabalome:
The study of the small molecules in the body.
Nanostring:
Measures gene expression changes during treatment.
GENIE (Genomic Expression by Nanostring: Inflammation Explained):
Genomics/transcriptomics testing:
References
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC88922/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6843326/
- https://www.survivingmold.com/Publications/CIRS_diagnostic_protocol_final_5_1_2018.pdf
- https://www.hoffmancentre.com/wp-content/uploads/pdfs/am/Chronic_Inflammatory_Response_Syndrome.pdf
- http://www.vaneuropsychiatry.org/mri-brain-volume-analysis/?utm_source=surviving%2Bmold&utm_medium=website&utm_campaign=survivingmold
- https://www.semanticscholar.org/paper/Intranasal-VIP-safely-restores-volume-to-multiple-Shoemaker/47f842701e3ac8e6340e58dace1338cabe5f0ecb
- https://www.sciencedirect.com/science/article/abs/pii/S0892036214001329?via%3Dihub
- https://www.hoffmancentre.com/wp-content/uploads/pdfs/am/Chronic_Inflammatory_Response_Syndrome.pdf
- https://hoffmancentre.com/chronic-inflammatory-response-syndrome-cirs-evaluation-and-treatment/
- Luger TA, Scholzen TE, Brzoska T, Bohm, M. New insights into the functions of alpha- MSH and related peptides in the immune system. PMID: 12851308
- Brozoska T, Luger TA, Maaser C, Abels C, Bohm M. Alpha-melanocyte stimulating hormone and related tripeptides: biochemistry, anti-inflammatory and protective effects in vitro and in vivo, and future perspectives for the treatment of immune-mediated inflammatory diseases. Endocrine Reviews. 2008;29(5):581-602.
- Lipton JM, Catania, A. Mechanisms of anti-inflammatory action of the neuroimmunomodulatory peptide alpha-MSH. PMID: 12470216
- Kriegel MA, Ming LO, Sanjabi S, Wan YY, Flavell RA. Transforming growth factor-beta: recent advances on its role in immune tolerance. Current Rheumatology Reports. 2006;8:138-144.
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6566291/
- Sorensen B, Jones JF, Vernon SD, Rajeevan MS. Transcriptional control of complement activation in an exercise model of chronic fatigue syndrome. Molecular Medicine. 2009 Jan-Feb;15(1-2):34-42
- https://www.hoffmancentre.com/wp-content/uploads/pdfs/am/Chronic_Inflammatory_Response_Syndrome.pdf
- Candelario-Jalil E, Thompson J, Taheri S, Grossetete M, et al. Matrix metalloproteinases are associated with increased blood-brain barrier opening in vascular cognitive impairment. Stroke. 2011 Mar 31. [Epub ahead of print] PMID: 21454822
- https://www.hoffmancentre.com/wp-content/uploads/pdfs/am/Chronic_Inflammatory_Response_Syndrome.pdf
- Candelario-Jalil E, Thompson J, Taheri S, Grossetete M, et al. Matrix metalloproteinases are associated with increased blood-brain barrier opening in vascular cognitive impairment. Stroke. 2011 Mar 31.
- Labcorp definition
- Alonso G. Vasopressin and angiogenesis. Journal de la Société de biologie. 2009;203(1):39- 47.
- Tansey KE, Hill MJ, Cochrane LE, Gill M, et al. Functionality of promoter microsatellites of arginine vasopressor 1A (AVPR1A): implications for autism. Molecular Autism. 2011 Mar 31;2(1):3 [Epub ahead of print] PMID: 21453499
- From Medline
- Olfert IM, Howlett RA, Tang K, Dalton ND, et al. Muscle-specific VEGF deficiency greatly reduces exercise endurance in mice. Journal of Physiology. 2009 Apr 15;587:1755- 1767.
- https://www.hoffmancentre.com/wp-content/uploads/pdfs/am/Chronic_Inflammatory_Response_Syndrome.pdf
- Delgado M, Gonzalez-Rey E, Ganea D. Vasoactive intestinal peptide. Annals of the New York Academy of Sciences. 2006 Aug 2;1070:233-238.
- From Nutrition with Judy’s CIRS overview.
- https://jbiomedsci.biomedcentral.com/articles/10.1186/s12929-018-0410-z more under Papers
- Directly from Nutrition with Judy’s overview of CIRS
- https://www.ninds.nih.gov/health-information/disorders/postural-tachycardia-syndrome-pots#toc-what-is-postural-orthostatic-tachycardia-syndrome-pots-
- https://med.stanford.edu/pans.html
- https://pubmed.ncbi.nlm.nih.gov/16525752/
- https://acsess.onlinelibrary.wiley.com/doi/abs/10.2136/sssaspecpub63.2014.0043.5
- https://iovs.arvojournals.org/article.aspx?articleid=2268605
- https://hoffmancentre.com/chronic-inflammatory-response-syndrome-cirs-evaluation-and-treatment/
- https://hoffmancentre.com/chronic-inflammatory-response-syndrome-cirs-evaluation-and-treatment/
- https://www.ncbi.nlm.nih.gov/books/NBK459455/
- https://www.ncbi.nlm.nih.gov/books/NBK21070/
- https://www.ncbi.nlm.nih.gov/books/NBK27100/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3134601/
- https://www.progenedx.com/methods
- https://www.progenedx.com/methods